
Preventing Gun Violence Starts in the Waiting Room
Each patient intake form functions as a form of decision architecture. It guides the patient on which health-related issues are relevant and informs the provider about which topics to discuss. Essentially, it establishes the boundaries of the conversation before any dialogue begins.
Smoking. Alcohol. Seatbelts. Sunscreen. These questions feel routine because forms made them routine. Nobody bristles when their doctor asks how many drinks they have per week. That normalcy was deliberately designed.
So, what happens when a leading cause of death never makes it onto the form?
The research.
During my graduate studies, I conducted an IRB-approved study examining how healthcare providers approach one of the most consequential (and most avoided) topics in patient care: firearms in the home.
The study had two parts. I interviewed practicing medical professionals about whether, when, and how they discuss gun safety with patients. I also conducted a content analysis of 93 publicly available patient medical history forms from practices across the United States, coding each form for eleven common lifestyle and social history questions. including everything from tobacco use to sun protection.
What I found was a gap. Not a gap in caring. A gap between what providers believe and what the system around them permits them to say.
One question is missing.
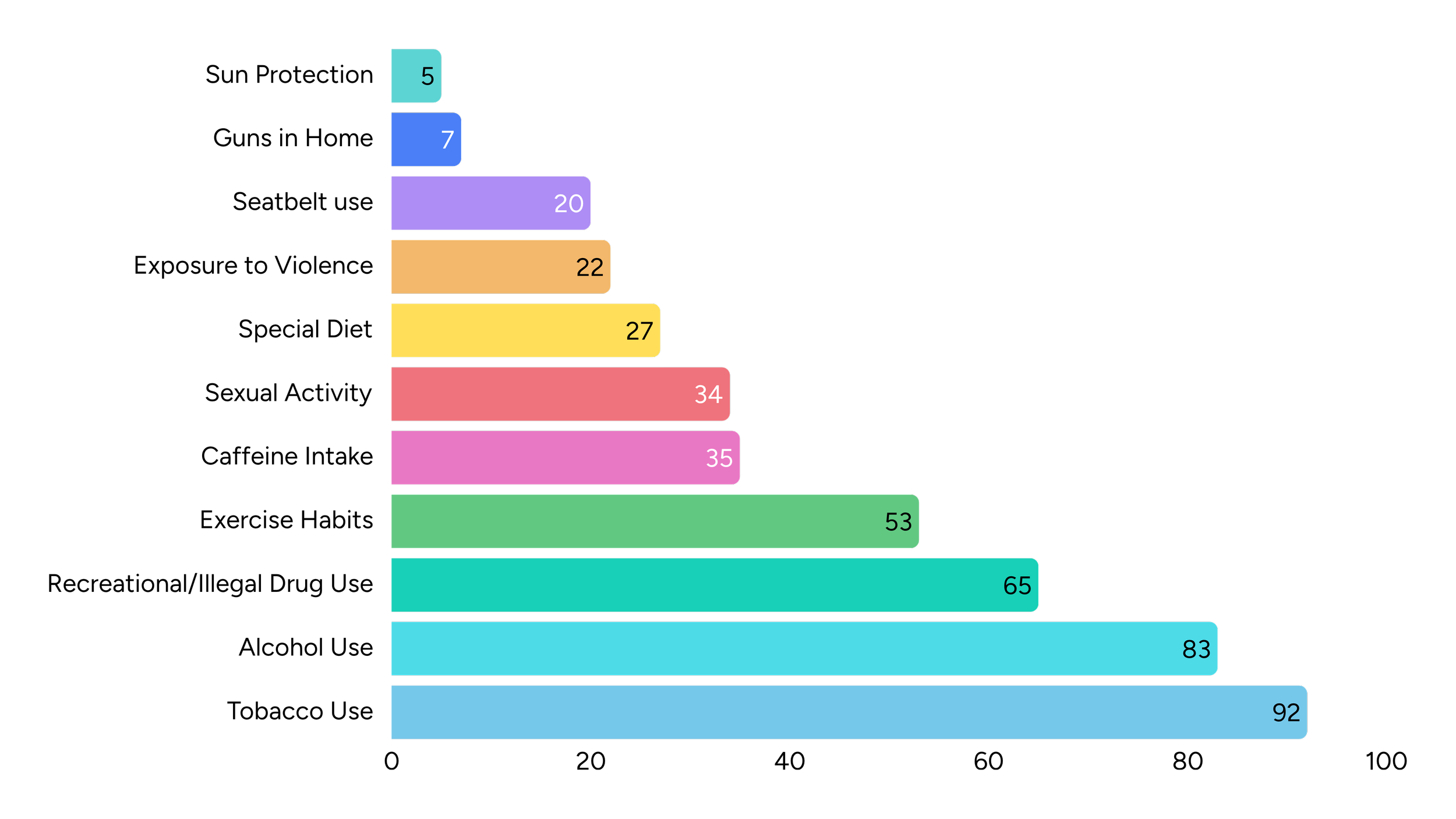
Questions about tobacco use appeared on 98.9% of the forms I analyzed: alcohol, 89.2%. Even seatbelt use appeared at 21.5%.
Questions about guns in the home appeared on 7.5%.
The only topic asked about less often than firearms was sunscreen.
Sit with that comparison. In 2024, more than 44,000 people in the United States died from gun-related injuries, and roughly six in ten of those deaths were suicides, deaths in which access to a firearm during a moment of crisis is one of the most significant risk factors we know of (CDC, 2024). Meanwhile, 38% of intake forms asked about caffeine (Figure 1). Rightly so. Caffeine interacts with sleep, anxiety, other health conditions, and some medications. That's exactly the point: the form already asks about modest, manageable risks because they're relevant to care. By that standard, the firearm question isn't a new idea. It's an overdue one.
Figure 1. Frequency of lifestyle questions by category as found on patient medical history forms
Everyone agreed gun violence was a crisis.
Here is the finding that reframes everything above: the missing question is not a belief problem.
Every provider I interviewed agreed — immediately, unanimously, and without hedging — that gun violence is a public health crisis. Their answers to that question were one word long. And yet only one of them routinely asked patients about firearm access, and only because she had folded it into a standard intake process at a previous practice.
Communication research has a name for this: the gap between attitude and behavior. Believing something matters is not the same as acting on it, and the distance between the two is where most well-intentioned health initiatives quietly die. My interviews surfaced exactly what fills that distance for providers:
Fear of being misread. Providers worried that asking about guns would be heard as a political statement rather than a clinical one, and that a routine safety question would land as an accusation or a threat to their right to possess firearms. One took deliberate care to ask about firearms with the same neutral tone she used for illicit drug use, precisely to strip the question of any perceived bias.
Role confusion. Nearly everyone believed the conversation was someone else’s. Specialists pointed to primary care. Primary care pointed to psychiatry. When responsibility is everywhere, it is nowhere.
Selective triggers. In practice, the question surfaced only when a patient showed visible signs of a mental health crisis, and even then, often only if the patient described a specific plan to harm themselves or others. Demographics quietly filtered who got asked, too: younger patients were read as “higher risk,” while elderly patients were rarely asked at all.
Provider safety. The most sobering barrier was the least expected: some providers have reason to fear the topic physically. One described leaving bedside care in part because searching patient belongings meant risking an encounter with a weapon. Her hospital now posts stickers on its doors reminding visitors that guns are not allowed inside, a warning she found surreal in a building meant to be among the safest places in the world.
None of these barriers is a lack of conviction. They are friction: social, structural, and situational. And friction is a design problem.
How a form field changes behavior.
Three frameworks from behavioral science explain why something as small as a printed question can close the gap between attitude and action.
The Health Belief Model tells us that people rarely act on health risks, even ones they take seriously, without a cue to action: a prompt that surfaces the issue at the right moment. A reminder card. A question from a doctor. A line on a form. For providers, the intake form is that cue.
The Theory of Planned Behavior adds that behavior follows not just from attitudes but from subjective norms, what we believe others will approve of, and from perceived control. The providers I interviewed did not lack the right attitude. They lacked normative cover. A question printed on the standard form supplies it: this is not my agenda, it is simply what we ask. The form converts a personal choice into an institutional norm.
The Stages of Change model reminds us that people move toward new behaviors gradually — from not considering a change to contemplating it to acting on it — and that a well-placed prompt can move someone from one stage to the next. My interviews captured this in miniature: providers who had never considered the question were, by the end of a single conversation, actively reconsidering their practice.
Theory is one thing. Watching it work is another.
The provider who routinely asked about firearms had discovered the mechanism on her own: she streamlined the gun question into her standard safety questions, right between sunscreen and seatbelts, so it would carry no emotional charge. Her patients’ typical reaction? A shrug. In her words, most people didn’t care that she asked. The providers’ fears of offense, so vivid in the abstract, largely evaporated in the exam room when the question arrived as routine.
The most memorable moment of the research made the cue-to-action effect visible in real time. One provider, who works with elderly patients, including many with dementia, initially told me firearms weren’t relevant to her practice. As we talked, she paused and reconsidered, realizing in the moment that for a patient with dementia, a firearm in the home is a genuine safety risk, and that this had simply never occurred to her before. A single question, asked once, changed her clinical thinking mid-sentence.
That is what a cue does. And that is what the form fails to do 92.5% of the time.
Omission is a design decision.
We tend to audit what our communications say. We rarely audit what they don’t say. But in high-stakes environments, the omission is the message. A form that asks about sunscreen but not firearms implicitly but unmistakably tells providers and patients which risks are speakable.
The fix requires no legislation and virtually no budget. It is a line of text on a document that every practice already uses, and every patient already fills out. Public health has run this play before: tobacco, seatbelts, and safe sex all traveled the same road from unaskable to unremarkable, and routine screening questions helped pave it. Pediatrics has even mapped the route: the American Academy of Pediatrics already provides guidelines for discussing firearms in homes with children, and the providers I interviewed pointed to those guidelines as exactly the kind of institutional cover that makes the conversation possible. The infrastructure for normalizing a difficult conversation already exists. It’s sitting on a clipboard in every waiting room in the country.
Design for what goes unsaid.
At form + field, I approach communication as a system: one where the questions you ask, the order you ask them in, and the questions you leave out all shape behavior. Sometimes the highest-impact intervention isn’t an elaborate campaign. It’s a checkbox.
If your work involves making hard conversations possible in health, safety, or public trust, let’s talk about what your materials are quietly making normal, and what they’re leaving unsaid.
A note on the research: This study was conducted during my graduate work at George Mason University with IRB approval. It included one-on-one interviews with practicing medical providers and a content analysis of 93 patient medical history forms drawn from all four U.S. census regions, validated by a second coder (Cohen’s κ = .924). Provider details have been kept general to preserve participant confidentiality. National mortality figures above reflect 2024 CDC data.
Sources
1. Centers for Disease Control and Prevention, National Center for Health Statistics (2024 firearm mortality data).
2. Rosenstock, I. M. (1974). Historical origins of the Health Belief Model. Health Education Monographs, 2(4), 328–335.
3. Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50(2), 179–211.
4. Prochaska, J. O., DiClemente, C. C., & Norcross, J. C. (1992). In search of how people change: Applications to addictive behaviors. American Psychologist, 47, 1102–1114.
5. Frattaroli, S., Webster, D. W., & Wintemute, G. J. (2013). Implementing a public health approach to gun violence prevention: The importance of physician engagement. Annals of Internal Medicine, 158(9), 697–698.
6. Kellermann, A. L. (1997). Gunsmoke: Changing public attitudes toward smoking and firearms. American Journal of Public Health, 87(6), 909–910.
7. Graziano, M., & Pulcini, J. (2013). Gun violence and the role of health care: A confusing state of affairs. AJN, American Journal of Nursing, 113(9), 23–25.